Infiltrative-pneumonic lung tuberculosis considers as the phase of focus lung tuberculosis progression, at which infiltration and perifocal inflammation are leading. The source of infiltrative pneumonic process can be repeated exogenic infection. In this form of tuberculosis the tissue reaction of proliferation is extremely diverse in lungs. The mechanism and reasons of occurrence of different forms of infiltrations are complicated. As a rule the infiltrative pneumonic process development is based on hyperergic reaction of an organism, hypersensitizing of lung tissue, lability of vegetative innervations and endocrine systems.
The following types of infiltrative tuberculosis are distinguished:
- Broncho-lobular infiltration;
- Rounded infiltration;
- Cloudy infiltration;
- Periscissuritis;
- Lobitis;
- Caseous pneumonia.
Broncho-lobular infiltration (Fig 3.7.1. a) is a focus located in cortical fields of the top first or second lung segments. Such infiltrations have wrong rounded form, with indistinct contours, diameter 1-3 cm. At tomography it consists of 2-3 or several merged fresh focuses. Clinical signs are usually asymptomatic, without functional changes and mycobacterium expectoration.
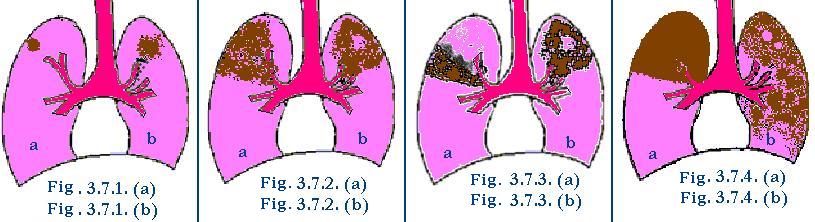
Rounded infiltration (Fig 3.7.1. b) represent itself as focuses of rounded or oval form, without sharp contour, in diameter of 1,5-2 cm, located more often in I-II or VI lung segments. From the focuses to the lung roots there is inflammative “path”, on which background the projection of bronchus is determined. It is possible to reveal on tomogram inclusions of more dense or calcified focuses, presence of fine cavities of disintegration, changes of pleura, scar formations. At progressing of round infiltrations there is an increase of a zone of perifocal inflammation, occurrence of signs of caseous disintegration of the focus with formation of a cavity. The cavity contains sequestrations and small amount of liquid pneumoniogenic cavity. Focuses of various sizes appear in healthy sites of lungs as a result of bronchogenic dissemination.
Cloudy infiltration (Fig 3.7.2. a) Cloudy infiltration. On X-ray film it is represented by non-uniform markings. The contours are diffused, distributed to one or several segments of the upper lung fields. Infiltration looks like picture on unspecific lobes pneumonia, but differs from it by stability of rentgenological changes, tendency to disintegration and formation of cavities (Fig 3.7.2. b).
Periscissuritis, or regional infiltration, of the triangle form is cloudy infiltration, located at interlobe fissure (Fig 3.7.3. a). The tip of a triangle is inverted to lung root, base– to peripheral. The top border is dim passing without sharp outlines in unchanged lung tissue. The bottom border corresponds interlobe pleura and consequently precise. On tomogram, the background has inflammatory infiltrations which come to light the shadows of more dense focuses, cavity of disintegration, rod and scar formations of condensed parenchyma.
Lobitis – infiltrative process extending on all lungs lobe (Fig 3.7.4. a). The lobitis differs by the structural forms (big quantity of caseous focuses) and aggravated clinical picture. The supervision of the course of this form of lung tuberculosis has shown that lobitis arise from development of small infiltration. On progressing of the process all lung lobe is affected, which is limited by precise interlobe fissure.
Caseous pneumonia.
In some individual patients with insufficient immunobiological stability infiltration converts to caseous pneumonia (Fig 3.7.4. b). Caseous pneumonia is characterized by development in lung’s tissue inflammative reaction with prevalence of caseation, in which connection caseous–pneumonic focuses on occupying up to a lobe or even a whole lung. Caseous pneumonia development is promoted by a number of the adverse factors: bad nutrition, pregnancy, diabetes, massive infection highly virulent MBT. Caseous pneumonia can be developed after pulmonary hemorrhage in result of blood aspiration contaminated by MBT. Pulmonary hemorrhage arises from lung cavity, which promotes distribution MBT healthy sites of lungs. The clinical signs of caseous pneumonia are determined by extension and intensity of morphological changes.
Clinical signs of infiltrative tuberculosis
The prominence of clinical signs of infiltrative lung tuberculosis as a rule corresponds to specific tuberculous damage in lungs. In most cases infiltrative pneumonia begins acutely with high temperature and can proceed as lobar pneumonia or influenza. The clinical signs of acute disease occur on a background of complete health. Only after careful examination of the patients it is possible to reveal symptoms like tubercular intoxication, appeared prior to the beginning of the disease onset. Quite often hemoptysis or bleeding is the first symptoms of infiltrative pneumonic tuberculosis. The duration of the acute period of the disease is various: it lasts from several days to several weeks. From the complaints are marked more often pains in a chest (in the damaged side or in area of a scapula), dry cough or cough with poor sputum expectoration. The phenomena of tubercular intoxication is expressed: bad appetite, sweating, disturbances of sleep, raised excitement, tachycardia, general weakness.
At caseous pneumonia beginning of disease is acute: with high temperature until 40-41° C, of hectic type, with the large differences between morning and evening temperature. Symptoms of tubercular intoxication quickly arise: the acute adinamia; profuse sweating, chest pains, cough with purulent sputum, dyspnoea are observed. Patients lose weight quickly. At physical examination, the initial signs of infiltrative tuberculosis are: at breath chest lagging in the side of the focus, stiff and painful chest muscles, strengthening of vocal vibrations.
The data of percussion and auscultation get more expressed character in massive pneumonia such as lobitis and at beginning disintegrations of infiltrations with cavity formation. At this time it is possible to determine above the defected site: dullness of percussion sounds, bronchophony, bronchial breathing, and crepitation of various characters. For diagnostics infiltrative pneumonia is very important the data of laboratory examinations. At this forms of tuberculosis, especially in a phase of disintegration, in sputum or in bronchial flush waters it is possible to find out MBT.
X-ray.
Radiologically the disintegration of infiltration is characterized by occurrence of sites of enlightenment. With increasing of their sizes, they get irregular, protruding form, surrounded by massive perifocal shadows blackout, so-called pneumogenic cavity. The size of cavities depends on the sizes of infiltrated disintegration. At X-rays examination of the patients with caseous pneumonia multiple, diffused, fused focuses are revealed of wrong form with dim contours. Progressing of the process results in formation of multiple cavities and occurrence of the focuses of bronchogenic metastastasis.
Differential diagnosis of infiltrations.
A sharp beginning of disease and fast development pneumonic process at the persons who are not having tubercular anamnesis, serve an occasion for statement of the diagnosis unspecific pneumonia. Especially difficult the diagnosis infitrative-pnumonic tuberculosis proceeding with influenzal syndrom. Important differntialy-diagnostic differences from pneumonia are:
- signs of tubercular intoxication;
- gradual beginnings of disease;
- absence of catarhal inflammation of upper breath paths;
- rather satisfactory condition of the patients, despite of high temperature.
At unspecific pneumonias with high temperature condition of the patients is serious, while the specific (tubercular) process proceeds with absence clinical signs at the beginning of disease and their occurrence only at progression of the process with formation of cavities. The results of blood analyses of the tuberculosis patients observes insignificant shifts in leucocytes formula and small acceleration ESR, to compare with croupous pneumonia, when high leucocytosis and sharply accelerated ESR take place.
General view X-ray examinations reveal that tubercular infiltration usually are mostly localized in upper parts of the lungs, but nonspecific inflammatory processes in lungs are more often arranged in middle and bottom fields. The tubercular infiltration is accompanied usually by “path” to the lung root; localized focus shadows could be visible on periphery of the basic tubercular focus. Such focuses cold be localized in other sites of the same lung or in opposite lung as result of bronchogenic dissemination. In some cases to ascertain diagnosis of tuberculosis only is possible after repeated investigation of patient’s condition; negative effect of treatment with nonspecific antibacterial drugs, revealing of MBT in sputum.
Long term inverse development of process allows to distinguish infiltrative-pneumonic lung tuberculosis from eosinophilic pneumonia due to the fact that main attribute of eosinophilic pneumonia is quick (during several days) resolution of the lung focus. Besides, at eosinphilic pneumonia, eosinophilia in blood reaches 30-45%. Eosinphilic pneumonia disappear without trace: after 7-10 days complete restoration of the lung tissue. Rather often the tumors (especially bronchogenic lung cancer resemble picture of infiltrative tuberculosis. The lung cancer developing from large broncus produces shadow of rounded form of infiltration.
In the blood analyses noteworthy monocytosis , sometimes eosinophylia and very high ESR. It is necessary to do tuberculin tests; if they are negative, it is possible to assume presence of a lung cancer. Finally diagnosis is put on the basis of all listed clinical symptoms.
Besides malignant neoplasms, tubercular infiltration sometimes it is necessary to differentiate with hydatid disease of lung, actynomycosis, lymphogranulomatosis, dermoid cyst, lung syphilis etc. Only detailed research of the patient and careful analysis of clinical, laboratory, roentological data data allow correctly to distinguish character of process in lung tissue.
Treatment.
The treatment of infiltrative tuberculosis begins in hospital conditions with application of most effective antibacterial drugs (1-st line) on a background of a pathogenic therapy. The treatment of the patient will be carried out up to complete resolution of infiltrative changes, on the average 1,5 year, followed anti-relapse out-patient treatment.
The clinical variety of the tuberculosis infiltrative pneumonia forms causes need of application of various ways of treatment. At absence of long effect and when destruction is not interrupted it could be useful to combine chemotherapy with collapse therapy (artificial pneumothorax).