Two basic forms of pleurisy are distinguished according to pathomorphological picture of tubercular inflammations of pleura: dry or fibrinous (pleuritis sicca, fibrinosa), and exudative (pleuritis exudativa). At dry, fibrinous pleurisy on chest x-ray the sites of diffuse of downturn of transparency are revealed, mainly in outside departments. On chest x-ray pleural effusion is defined as massive homogeneous opacity with slanting, quite often precise, top border. The size of a shadow depends on amount of liquid, therefore it can be from hardly noticeable appreciable as a small thickening of a costal edge up to significant, occupying the most part of lung fields. In such cases the displacement of mediastinum in the healthy part is usually marked.
If liquid accumulated above diaphragm, frequently is not visible at radiographic examination of the patient in a vertical position. In similar cases the examination in lateral position is necessary. Lung picture is differentiated poorly. The free liquid can move depending on a position of the patient’s body. Pleural exudates can accumulate in interlobe fissures in paramediastinal regions and in the field of diaphragm domes, where densities defined by various positions of the body at radiographic examination.
More difficult is radiographic diagnostics of encysted pleurisy, which shadow can have the different localizations. Encysted pleurisy can get encysted due to the presence of pleural adhesions. According to localization, pleurisy:differ into:
- costal-diaphragmatic;
- diaphragmatic;
- costal;
- interlobe;
- paramedistinal;
- apical.
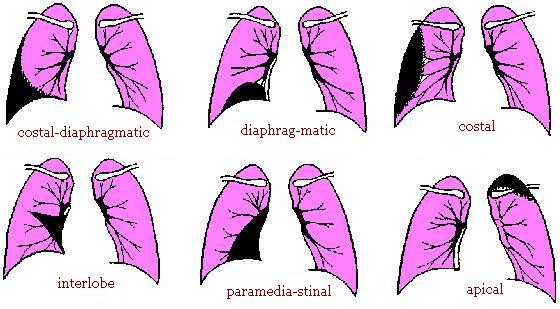
The encysted pleurisy differ by that at roentgenoscopy it is visible, that the liquid almost does not move at breath of the patient and change of body position. On anterior-posterior chest x-ray a shadow of high intensity is defined, of different size (depending of liquid quantity). The greatest importance for diagnostics of encysted pleurisy has lateral x-ray and tomograms.
Pleural thickenings are formed usually after exudative pleurisy, but could be met at many other forms of lung tuberculosis as a consequence of involving pleura in a process. Sites of reduced lucidity are defined, mainly in peripheral departments of lungs. On this background pleuro-pulmonic scars are found out freuently as rough linear shadows going from outside lung edge deep into it. Sometimes pleural thickenings are calcified. Then they are defined as a shadow of the very high intensity of the various form: a spots, linear formations, points. Pleural thickenings and pulmonic scars could be revealed not only at tuberculosis, but also at all inflammation lung diseases easy.