The inflammative changes in the lung and in the lymph nodes (lymphadenitis) and lymph paths (lymphangitis) are together known as the Primary tuberculosis complex. Thus, the picture of primary tubercular complex consists of three components: changes in the lungs, lymphangitis, and lymphadenitis.
In the second phase of dissolving (bipolarity) the reduction of perifocal zone of inflammation (3) is observed. The centrally located caseous focus is becoming more prominent. The signs of inflammation in regional lymphatic nodes (1) and of bronchi – vessels picture are decreasing.
In the third phase dissolving, give way to the phase of condensation: the primary focus is well outlined, its contours precise, on periphery of the focus there is a beginning of calcification as fine pieces; at peripheral regions of lung bronchial lymphatic nodes calcification is also present.
In the fourth phase, in the place of broncho-lobular pneumonia (3) calcification become compact, the focus gets rounded form and regular precise contours, its size does not exceed 3-5 mm. This formation if called Gohn’s focus.
Outcomes of the primary tubercular complex:
- the healing with encapsulation, calcification or ossification;
- progression with development of the various forms of the generalization, joining of unspecific complications such as atelectasis, pneumosclerosis and etc.
At progressing of the primary complex the hematogenic and lymphagenic-glandular generalization are distinguished.
The hematogenic generalization develops at MBT penetration into the blood. An obligatory condition for the hematogenic generalization is the hyperergic condition. Depending on condition of a primary tubercular complex differentiate early generalization, shown as:
- the general miliary tuberculosis with massive dissemination of the productive or exudative nodes in all organs;
- the macrofocal tuberculosis with formation of caseous focuses, with the size up to 1 cm.
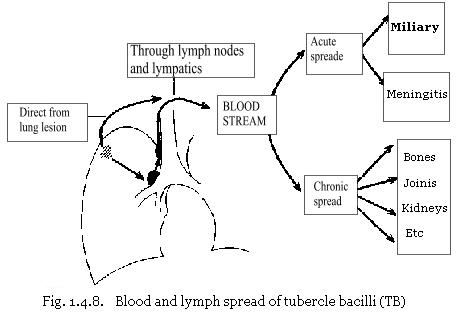
The focuses of hematogenic generalization can be source of development of the organic or of the general miliary tuberculosis at the relapse tuberculosis. Hematogenic tuberculosis more often arises at primary tuberculosis during dissemination of mycobacterium in the body (bacilemia). At the secondary forms of tuberculosis mycobacterium penetrate into blood stream from the exacerbated tubercular focuses located in lungs, lymphatic nodes, bones and other organs (See Fig. 1.4.8.).
The occurrence of tubercular bacilemia promoted by hypersencibilization and hyperergia of organism on ground of the specific infection, influenzas, allergic frustration, avitaminosis, infringement of proteins exchange. To hypersencibilization and formation of hematogenious lung tuberculosis exogenic super infection promotes at long and massive contact with bacillary patient. For development of disseminated forms of tuberculosis, the basic condition is the presence bacilli, and massiveness and virulence of infection. High importance has a condition of infected organism:
- Presence of contact (contact with sputum positive patient);
- Age of the patient (0-14, > 65 years);
- Diseases which patient survived in past, on which background the disseminated lung tuberculosis had developed.
For the adult, the important role working conditions play, condition of nervous system, consequences of heavy emotional shocks, former events of lungs or other organ tuberculosis. From foci of lymphatic nodes of the primary complex, at mycobacterium are distributed through lymphatic pathway, through thoracic duct and venous system of the right heart, causing isolated mycobacterium dissemination in a small blood circulation, that is, in lungs. During mycobacterium penetration into lung veins, MBT penetrate to the left heart and after into peripheral vessels of systemic circulation, causing damage of different organs (See Fig. 1.4.8.).
At progression of hematogenious disseminated tuberculosis the cavities are formed. The formation of cavities is the result of cheesy disintegration and dissolution of necrotic masses. The cavities are usually thin-walled, multiple and settled down symmetrically in both lungs. In an origin of such cavities plays important role damage of blood vessels, their thrombosis and obliteration. The poor blood supply of these focuses in lungs and their destruction is formed resembling trophic ulcers. The formation of cavities the opens the possibility of bronchogenic dissemination of healthy regions of lungs. Hematogenic dissemination of mycobacterium is always combined with lymphogenic. Thus MBT not necessarily penetrate into the blood at one time owing to break of the large focal necrosis. They can penetrate repeatedly by small portions, passing in the beginning through lymphatic vessels. Such genesis gives different clinical and rentgenological display of heamatogenic disseminated forms with various courses, duration of the disease and with heavy outcome or recovery.
The lymphogenic forms of disseminated tuberculosis usually arise at an aggravation of the focuses and of the small cavities in lungs. Mycobacterium tuberculosis penetrates into nearby lymphatic vessels, as consequence, the dispersed focuses, sometimes tubercles and productive type, lymphangitis develops. In the process frequently visceral pleura is involved. The groups of the defeated lymphatic nodes (caseous lymphadenitis) are increased in the sizes, merge in conglomerates, grow together with nearby organs (bronchi, vessels, nerves, pericardium), squeeze them, cause various functional infringements. The glandular tubercular focuses are poorly accessible to action of antibacterial drugs, and are the source of serious complications: such as distribution of the tubercular process on the mediastinum organs; joining of a secondary infection; development of amyloidosis of internal organs. The growth of the primary focus can be observed at lymphoglandular generalization, and also as the independent form of disease. To the heaviest progressing forms of the primary focus concern: caseous pneumonia with formation of the disintegration cavity and primary cavity. From the moment of the cavity formation the bronchogenic dissemination switched on and as the consequence of this process in both lungs develop focuses of tissue reactions develop of various sizes and type. The cavitations of the focuses of the caseous pneumonias comes to an end as «primary lung phthisis».
For chronic primary lung tuberculosis are typical:
- the caseous necrosis of lymphatic nodes;
- predisposition to hematogenic dissemination with development of out-lung metastatic focuses and regional to them the lymphatic nodes inflammation;
- the polyserositis.
Rarely, the primary lesion may progress directly to the post-primary form characterized by extensive caseation necrosis and cavitation. More commonly, the primary lesion remains quiescent and may remain so for decades or for the remainder of the individul’s life time. The precise mechanisms underlying this phenomenon have not yet been clarified as yet. However, reactivation or reinfection tuberculosis may occur due to old age, malnutrition, malignant disease, HIV infection and acquired immunodeficiency syndrome [AIDS], use of immunosuppressive drugs and intercurrent infections.